
{kind=link}
[ad_1]

By Christine H. Monahan and Linda J. Blumberg
As hospitals increase in dimension and scope, together with taking on outpatient well being care settings, costs for routine medical companies are rising, typically dramatically. This is an issue in each Medicare and the industrial insurance coverage market as a result of hospitals usually invoice further facility charges on high of the skilled prices from the physicians or different practitioners who present care. In the industrial market, the results of facility payment billing are compounded by the shortage of value regulation limiting how a lot market-dominant hospitals and well being programs can cost. The rising dimension of deductibles, in addition to extra, distinct cost-sharing obligations for hospital and doctor payments, imply that buyers usually instantly bear the brunt of those prices.
Over the previous a number of years, Congress and the Centers for Medicare and Medicaid Services (CMS) have taken preliminary steps to rein in facility payment billing in Medicare, however a lot of the issue stays. Today, Congress is contemplating a number of proposals (exhibit 1), most of that are bipartisan, to maneuver the ball ahead one other step. In this text, we take a more in-depth have a look at the present slate of proposals to reform abusive billing practices within the industrial market.
Exhibit 1: Current congressional proposals to reform or enhance transparency on facility payment billing below industrial well being plans
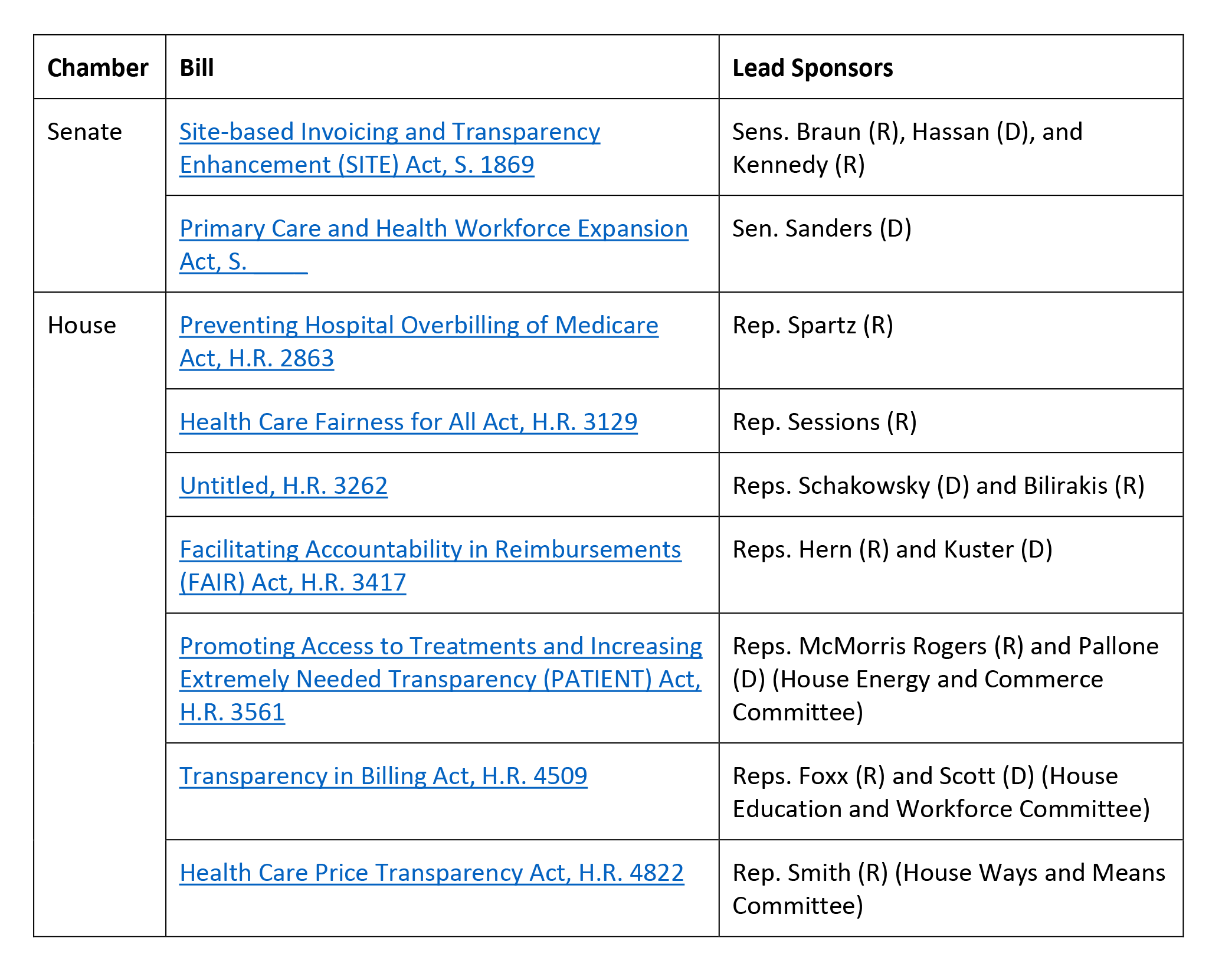
Source: Authors’ evaluation.
Price Caps And Site Neutrality In The Commercial Market
By far, essentially the most complete invoice floated so far is Senator Bernie Sanders’ (I-VT) Primary Care and Health Workforce Expansion Act. What makes this invoice stand out is that it seeks to not solely curtail abusive outpatient facility payment billing within the industrial market, as some states have begun to do, but in addition would impose value caps as a mechanism to attain site-neutral funds for a significant swathe of companies.
We have beforehand mentioned the constraints of prohibiting outpatient facility payment prices with out together with extra pricing constraints. In quick, prohibiting hospitals from billing outpatient facility charges with none regulation of the overall costs charged permits hospitals with market energy to extend the charges their affiliated physicians and different well being care professionals cost for these companies and in any other case enhance costs for different companies to make up for the misplaced income. Although such reforms could generate short-term financial savings, they’re unlikely to meaningfully include prices within the longer run. Adding value caps, a minimum of for a specified set of low-complexity outpatient companies generally supplied in doctor places of work, would restrict hospitals’ potential to extend skilled charges for outpatient companies past a specified degree. How excessive or low that fee is relative to current reimbursement ranges, in addition to how broadly it applies, will largely decide the potential value financial savings. These value caps finally could lead insurers to attain “site neutrality,” paying the identical quantity for companies whether or not in a hospital or unbiased setting.
Sen. Sanders’ proposed value caps would attain a comparatively broad set of companies: all care supplied in off-campus outpatient settings in addition to low-complexity companies supplied in on-campus settings, as long as they are often safely and appropriately furnished in off-campus settings as nicely. This explicitly consists of analysis and administration companies and telehealth companies, in addition to different gadgets and companies to be decided by the secretary of Health and Human Services. This focus is just like proposals for site-neutral funds in Medicare from the Medicare Payment Advisory Commission and for limiting facility charges from the National Academy for State Health Policy.
In proposing a fee degree for these companies within the industrial market, Sen. Sanders is breaking new floor whereas drawing on an current idea: the No Surprises Act’s (NSA’s) qualifying fee quantity (QPA). Specifically, Sen. Sanders’ proposal would restrict suppliers and amenities to charging one payment that’s no better than the QPA for a coated merchandise or service. This side of the invoice is bound to ask debate; the calculation of the QPA below the NSA has confronted ongoing lawsuits by well being care suppliers and their supporters. It stays to be seen whether or not reliance on the QPA—and even the industrial value ceiling proposal extra broadly—survives past this primary draft of Sen. Sanders’ invoice (which has but to be formally launched), however, even when not, Sen. Sanders has opened the door to dialogue and debate of a coverage strategy that warrants consideration.
Transparency In Billing
The remaining industrial market billing reforms in Congress deal with enhancing transparency round outpatient facility payment billing. These proposals are pushed by a rising recognition that well being care payers, and the researchers, regulators, and coverage makers who depend on claims knowledge, have a surprisingly poor understanding of the place care is supplied, by whom, and at what complete value. For instance, claims varieties usually solely embrace the handle and nationwide supplier identifier (NPI) for hospital’s foremost campus or billing workplace somewhat than the off-campus web site of care. Discrepancies between the data on hospital claims (historically the UB-04 kind, or the digital equal thereof) {and professional} claims (historically the CMS-1500 kind, or the digital equal thereof) additionally make it troublesome to reliably affiliate hospital {and professional} payments for the service to determine the overall value of care. Additionally, outdoors of registries in particular person states equivalent to Massachusetts, there’s a lack of publicly out there knowledge monitoring hospital possession and management over outpatient suppliers and settings.
As a results of these info gaps, even insurers with some market leverage could also be unable to successfully negotiate with suppliers on the overall value paid for companies and can’t assess how a lot care is being supplied in numerous settings and the way the prices examine throughout these settings. Insurers additionally could have extra issue capitalizing on new legal guidelines, equivalent to in Texas, that prohibit anti-steering or anti-tiering clauses if they can’t reliably distinguish when care is being supplied at completely different outpatient places owned by the identical well being system. Additionally, absent higher info, coverage makers face challenges evaluating the potential results of various reforms, and regulators could have issue imposing new legal guidelines looking for to rein in abusive outpatient billing practices.
The majority of the presently pending payments largely search to deal with the shortage of location-specific info for the location of care on claims varieties. They all would require that hospital outpatient departments, as outlined by CMS below the Medicare program, acquire a novel NPI and use this identifier for billing. This 10-digit code would allow payers and different analysts reviewing claims knowledge to know the particular location the place care was supplied, with out the identical danger of errors that counting on an handle alone would introduce. (Additionally, merely requiring the placement’s handle with out updating the NPI could lead to insurer programs rejecting the claims as a result of the handle on the declare doesn’t match the handle related to the listed NPI.)
To the extent billing transparency laws strikes ahead, Congress might want to iron out technical variations among the many current proposals. One challenge is whether or not simply hospitals and amenities want to incorporate the location of care’s distinctive NPI on claims or if well being care professionals should embrace this info as nicely. Most of the laws focuses on hospital payments, however this misses out on an vital alternative. If the location of care’s distinctive NPI is persistently included on each hospital payments {and professional} payments, insurers and different analysts shall be higher capable of affiliate claims for a similar service and calculate the overall value of take care of every.
Both the House Energy and Commerce Committee proposal from Representatives Cathy McMorris Rodgers (R-WA) and Frank Pallone (D-NJ) and the House Ways and Means Committee proposal from Representative Jason Smith (R-MO) require the distinctive NPI on Medicare billing varieties solely. Representative Pete Sessions’ (R-TX) Health Care Fairness for All Act requires solely that off-campus hospital outpatient departments purchase a novel NPI however doesn’t explicitly require that it’s used when claims are submitted. In distinction, different proposals explicitly lengthen the requirement to be used of a novel NPI such that industrial claims can’t be paid with out it. Some, such because the Education and Workforce Committee’s invoice, even impose parallel necessities that insurers can’t pay and customers are usually not accountable for claims that don’t embrace the placement of care’s distinctive NPI.
Arguably, even a proposal that’s targeted on Medicare may gain advantage the industrial market as a result of rules below the Health Insurance Portability and Accountability Act (HIPAA) require well being care suppliers to make use of their NPI on all commonplace transactions. Nonetheless, there may be cause to consider payments explicitly extending this requirement to industrial claims and offering extra enforcement mechanisms might have higher compliance, and thus an even bigger impression. First, suppliers doubtlessly might argue that their unique, systemwide NPI remains to be legitimate and proceed to make use of that on industrial claims. Second, industrial insurers would want to replace their claims processing programs to just accept claims with the brand new distinctive NPIs, and so they could not discover the inducement to be sufficiently robust to take this step if the laws applies solely to Medicare billing. If Congress finally pursues a Medicare-only reform, it might behoove CMS to amend the HIPAA rules or challenge steering to make sure the brand new, distinctive NPI is required on all industrial claims as nicely and push insurers to accommodate these modifications.
While switching to distinctive NPIs is a important step to higher understanding location knowledge, it could turn into tougher for payers and researchers to see the system affiliation of the completely different places that are actually submitting claims. Payers and the broader public would considerably profit from a complete federal system for monitoring hospital possession and acquisitions, equivalent to that proposed by Representatives Janice Schakowsky (D-IL) and Gus Bilirakis (R-FL). Ideally this technique could be designed to enrich the distinctive NPI requirement, in order that hospitals and well being programs should report all of their affiliated distinctive NPIs and replace this info on a well timed foundation, on high of different knowledge necessities presently included within the invoice. To the extent such a proposal isn’t adopted, CMS ought to take into account how else it might be able to higher accumulate this info below current authorities—both leveraging knowledge collected as a part of the NPI utility or maybe newly accumulating such info by hospitals’ Medicare value experiences.
Looking Forward
The value penalties of present billing practices are substantial. Consumers want lawmakers to start curbing this abusive habits that places them liable to greater value sharing and medical debt and will increase their premiums. The proposals pending earlier than Congress are a important first step, though outdoors of Sen. Sanders’ invoice, they’re additionally solely that—extra targeted on transparency of knowledge on pricing than on decreasing complete costs of low complexity companies.
Assuming we don’t see vital expansions within the scope of those proposals in no matter bundle, if any, strikes ahead, it can fall on CMS, the states, and personal payers to maintain transferring the system ahead within the quick time period. But we should always not overstate the impression most of those proposals are more likely to have: Insurers in noncompetitive supplier markets have little to no leverage in negotiating decrease costs for companies, even when they’re able to acquire higher info on pricing. States are beginning to deal with this challenge however face vital opposition from the hospital business. What’s extra, the first tactic states have pursued so far—prohibiting facility payment prices for sure outpatient companies/settings—can lower shopper out-of-pocket prices however won’t scale back complete prices as market-powerful hospitals make up their prices elsewhere, and premiums rise accordingly.
Ultimately, limits on complete costs for outpatient care, together with facility {and professional} prices, are essential to eradicate the expansion in these ballooning billing practices which have unfold broadly as a consequence of vertical integration in well being care.
Authors’ Note
On Wednesday, September 6, 2023, as this text went to manufacturing, Axios revealed a dialogue draft floated by Republicans from the House Ways and Means, Energy and Commerce, and Education and Workforce Committees that might require Medicare hospital outpatient departments to acquire a novel NPI and use this for Medicare billing functions. The invoice is predicted to be launched imminently.
This publish is a part of the ongoing Health Affairs Forefront sequence, Provider Prices within the Commercial Sector, supported by Arnold Ventures.
Christine H. Monahan and Linda J. Blumberg, “Reforming Abusive Billing Practices, One Step At A Time,” Health Affairs Forefront, September 8, 2023, https://www.healthaffairs.org/content/forefront/reforming-abusive-billing-practices-one-step-time. Copyright © 2023 Health Affairs by Project HOPE – The People-to-People Health Foundation, Inc.
[ad_2]