
[ad_1]
A Health Affiairs Forefront article by DiGiorgio (2023) argues the 340B has outlived its functions. He writes:
By mandating that drug corporations give a big low cost to coated entities, nearly all of that are hospitals with disproportionate share or vital entry designations, the 340B program was meant to offer a monetary buffer for establishments such because the one the place I work. However, the 340B program has change into gamed by massive companies to extend income. It is not serving its authentic intent.
The program has grown quickly amongst hospitals that serve wealthier affected person populations. 340B hospitals are increasing into extra prosperous neighborhoods, and they’re conscious of payer combine as they transfer into areas with fewer publicly insured sufferers. 340B establishments usually tend to keep away from counties with decrease revenue ranges and extra uninsured sufferers. While Rep. Waxman argues that these revenues are getting used to extend service traces for low-income sufferers, the proof recommend that 340B hospitals didn’t improve look after underserved populations or improve their charges of uncompensated care. There are many reforms that would protect safety-net funding whereas curbing abuses of the 340B system
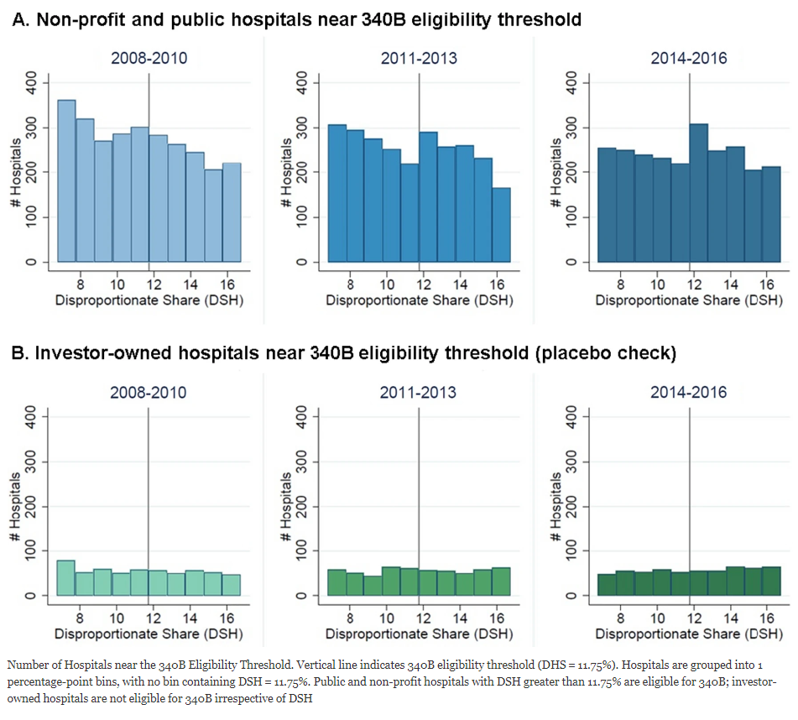
One key piece of proof DiGriogio cites is a paper by Mulligan et al. (2021). This examine discover strategic conduct amongst hospitals. Hospitals that recieve disproportionate share hospitals (DSH) funds are eligible for 340B if their DSH adjustment–a measure that identifies hospitals that deal with a disproportionate share of low revenue Medicare or Medicaid sufferers–is above 11.75%. Mulligan and co-authors used knowledge from Healthcare Cost Report Information System (HCRIS) to look at if hospitals are adjusting their DSH to achieve eligibility. Because investor-owned hospitals should not eliigble for 340B, one would anticipate no strategic conduct from these hospitals. The authors use a McCrary density exams to evaluate whether or not the noticed distinction in density of hospitals just under and above the 11.75% threshold was considerably bigger than what can be anticipated by probability alone. The authors discover that:
In 2014–2016, the variety of hospitals will increase by 41% simply above the 340B eligibility threshold. McCrary density exams discovered this improve to be statistically vital throughout a spread of bandwidths in 2014–2016 (p < 0.01)…We discovered no comparable change amongst hospitals ineligible for the 340B program. These knowledge are in line with the speculation that some hospitals modify their DSH to achieve 340B eligibility.
{kind=link}
You can learn the total Mulligan et al. (2021) paper right here.
[ad_2]